Laboratory testing has grown from a manual, “hands-on” process providing a simple test menu — with staff organized by testing methodology or discipline in multiple small rooms — to an automated, multidisciplinary, high-volume instrument-centric clinical enterprise. A visit to a hospital laboratory today reveals a varying array and number of instruments, often operating with little human intervention. While test volume and staffing were once used to determine the amount of space in a laboratory, today, the instruments and degree of automation dictate the test volume capacity. The number of staff required to support the instrumentation is then determined.
The following ten key questions should be addressed prior to planning space for a hospital-based laboratory:
What laboratory services will be provided? Although a full-service laboratory will include outpatient specimen collection, central specimen processing, core clinical laboratory, transfusion services (blood bank), microbiology, molecular diagnostics, and anatomic pathology, most healthcare centers will not need all of these components. In fact, many hospitals only need a central specimen processing area, a highly automated core laboratory to provide quick turnaround testing (with hematology, chemistry, coagulation, and urinalysis), and a blood bank. Some laboratories may operate an aggressive outreach program involving marketing and selling tests to physicians’ offices, other hospitals or clinics, nursing homes, veterinarians, and other organizations. A courier service is used to pick up the specimens and bring them back to the laboratory for testing. Space must be provided for specimen receiving and processing, courier management, and supplies, along with convenient parking and easy laboratory access.
How will specimens flow through the laboratory? Most specimens are either carried into the specimen processing section by couriers, hospital staff, or phlebotomists, or arrive via a pneumatic tube. Pneumatic tubes are used in most U.S. hospitals to transport of blood and urine specimens, as well as blood products and tissue samples. Specimens and paperwork may also be transported by autonomous mobile transport robots. Specimens move through specimen processing into testing areas and most are stored for a period of time (typically a week) before they are discarded. Anatomic pathology and microbiology specimens, and frozen sections and gross anatomy specimens from the surgical suite, may be taken directly to the respective testing area.
What instrumentation and automation is planned? The instrumentation required to perform the test menu in the laboratory, and the degree of automation, are the primary drivers of space. In the automated laboratory, a very large volume of tests can be performed on one analyzer run by one person. Full automation lines can connect many analyzers and require very little staff interaction other than loading them and making sure supplies are sufficient. Each instrument requires space for the instrument itself, supporting computers and printers, and an open area to hold and prepare samples.

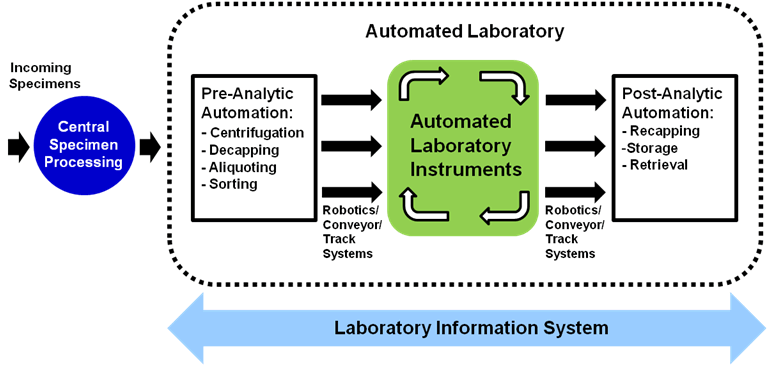
Clinical laboratory automation also involves the integration or interfacing of automated or robotic transport systems, analytical instruments, conveyor or track systems, and pre- and post-analytical process equipment such as automated centrifuges, decappers, aliquoters, recappers, sorters, and specimen storage and retrieval systems. In addition to the electrical and mechanical interfaces of these various components, the computers that control them must also be interfaced to each other and the laboratory information system. The vendor specifications will dictate the footprint, appropriate clearances, and supporting infrastructure and, in the case of a total laboratory automation system, the vendor may assist with the design and layout of the space.
What front-end automation will be used? Preparation of samples for testing includes receiving them into the laboratory information system to verify and confirm the orders and labeling. Depending on the level of automation in the laboratory, the specimens will either be placed on the automation line for front-end preparation, or manually centrifuged, aliquoted, and sorted into racks. From a facility planning perspective, this automation should run directly from where specimens are received to the testing areas.
How will specimens be stored? Archived specimens can be placed in a centralized area, such as a walk-in refrigerator in the specimen processing area, or in a refrigerator in the section where testing is done. In fully automated laboratories, the archiving can be part of the automation line. This will not eliminate the need for space to archive the non-automated testing and the spillover as the automated equipment reaches capacity. The overall space need will depend on the type and volume of tests being performed and the standard time the specimens are retained. When the specimens are no longer needed, they must be discarded into biohazard bags for disposal. In small laboratories, red bag receptacles may suffice; in larger facilities, a separate biohazard storage room will be necessary.
How much bulk storage space is required? Refrigerated and room temperature storage is required for reagents and supplies. The amount of space required for storage will depend on the size of the laboratory and the materials management procedures deployed.
Where will outpatient specimen collection occur? With hospital-based outpatient services increasingly centralized to enhance patient convenience and expedite treatment, outpatient specimen collection is routinely co-located with other outpatient services. Alternately, outpatient specimen collection may be performed at the point-of-care — within a physician office, clinic, or specialty treatment area. A small phlebotomy area may be provided within the hospital laboratory to be used during hours when outpatient areas are closed.
Where else will testing occur? The proliferation of point-of-care testing in recent years adds another dimension of complexity to laboratory services planning. Immediate results are provided using tabletop analyzers and handheld devices at the patient bedside, in the emergency department, and in outpatient and other clinical areas which expedites patient care.
What type of education programs will be provided? Education programs — typically found in large hospitals or academic medical centers — may require a significant amount of space in the laboratory depending on the training programs offered. This may include classrooms, study areas, and administrative offices and workstations, as well as practice equipment for students in the technical areas.
What about the blood bank? Minimally invasive surgical techniques, along with new transfusion guidelines, have dramatically reduced the utilization of blood products within the hospital, which impacts the amount of space required for immunohematology and the storage of blood products.
ALL OF THIS REQUIRES INCREASED FLEXIBILITY
Laboratory automation continues to evolve, with more and more testing procedures placed on large analyzers and integrated with an automated system. Some technology and instrumentation is changing as often as every two months. New automated platforms are being introduced for microbiology and anatomic pathology that will transform the traditional layouts of these sections. The storage of specimens, slides, blocks, and supplies is also becoming more automated. Flexible casework systems, adjustable-height counter tops, and overhead utility systems, which allow rapid connections for gases, water, power, data, and air, without major renovation, are becoming standard in clinical laboratories. Over time, an open, flexible space facilitates transitioning into new technologies with increasingly higher-volume testing capabilities. As a result, less space and less staff may be needed.
See the related post Hospital Laboratories Face New Organizational Models.
This article is an update of a previous post.